Finally, a very effective way to address CIPN deficits in active and post-treatment chemo patients. Fortunately, the solution is available right now!!
While Ribbons PT is known for unparalleled lymphedema treatment, we also provide comprehensive rehabilitation for patients suffering from the effects of cancer and/or cancer treatment. One of the most common deficits is peripheral neuropathy caused by chemotherapy treatments (CIPN), most notably Taxane-based chemotherapy which includes paclitaxel (Taxol), albumin paclitaxel (Abraxane), and docetaxel (Taxotere), as well as platinum-based drugs (cisplatin, carboplatin, and oxaliplatin) manifests as numbness, paresthesia, pain, and/or burning, though motor dysfunction (typically weakness) and/or autonomic dysfunction can also occur. The reported prevalence of CIPN following neurotoxic chemotherapy is 20-51 %, but estimates vary considerably depending on the agents assessed, the severity threshold, and mechanism of detection; but because sensory symptoms are not overt, underreporting of both the prevalence and magnitude of CIPN is likely. Once present, regression of CIPN symptoms is slow. Lingering or permanent symptoms are common and can significantly impair quality of life.1
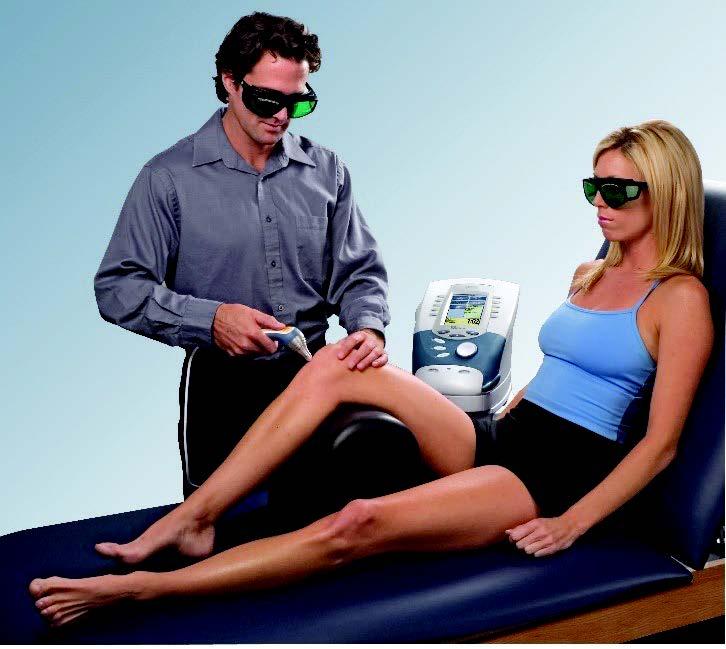
Cold Laser (Photobiomodulation/PBM, Low Level Laser Therapy/LLLT)
Photobiomodulation (PBM) also referred to as Low Level Light Therapy (LLLT) or “cold” laser, employs non-ionizing, low power, laser light therapy and has been shown in pre-clinical and small trials to improve neural function. 1 The term “cold” laser is used in that the beam does not generate heat. The laser head is at room temperature, so patients sensitive to cold are not adversely affected. PBM may improve neuropathy symptoms through a number of plausible mechanisms including prevention of neural apoptosis and enhancement of neurite outgrowth. Molecular level studies suggest that energy from low-level laser is absorbed by mitochondrial transmembrane proteins leading to: improved cellular respiration, and increased activation of oxidation-sensitive pathways including nuclear factor-KB and activator protein 1, which protect cells from apoptosis-promoting signals including tumor-necrosis factor-a, as well the JNK and lysosomal pathways. Zhang and colleagues reported differential expression of 111 genes after exposing human fibroblasts to PBM with more than half involved in cellular proliferation or suppression of apoptosis. In vitro study of human neural progenitor cells suggests laser light supports neurite outgrowth and whole animal studies of mice suggest significant improvement of functional recovery after nerve crush injury and platinum exposure using similar PBM strategies. 1

1. The effect of photobiomodulation on chemotherapy-induced peripheral neuropathy: A randomized, sham-controlled clinical trial by Peter A. Argenta, MDa et al
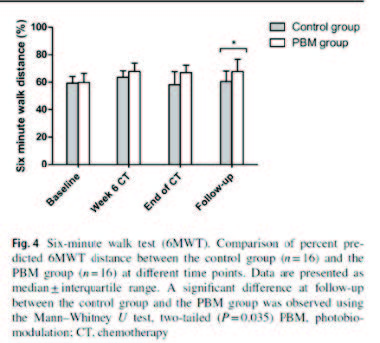
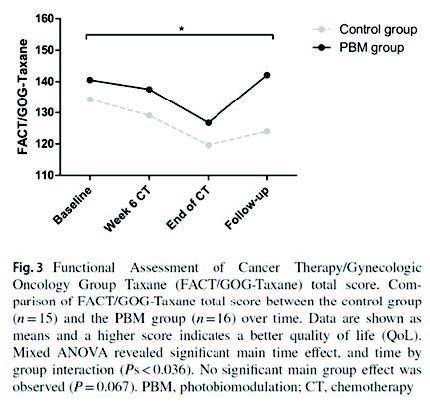
In one study, a prospective, randomized placebo-controlled pilot trial was set up with 32 breast cancer patients who underwent chemotherapy (ClinicalTrials.gov; NCT03391271). Patients were randomized to receive PBM (n = 16) or placebo treatments (n = 16) (2 x /week) during their chemotherapy. The modified Total Neuropathy Score (mTNS), six minute walk test (6MWT), Numeric pain Rating Scale (NRS), and Functional Assessment of Cancer Therapy/Gynecologic Oncology Group Taxane (FACT/GOG-Taxane) were used to evaluate the severity of CIPN and the patients’ quality of life (QoL). Outcome measures were collected at the first chemotherapy session, 6 weeks after initiation of chemotherapy, at the final chemotherapy session, and 3 weeks after the end of chemotherapy (follow-up). Results: The mTNS score increased significantly over time in both the control and the PBM group. A significantly higher score for FACT/GOG-Taxane was observed in the PBM group during chemotherapy compared to the control group. Questions of the FACT/GOG-Taxane related to sensory peripheral neuropathy symptoms showed a significant increase in severeness over time in the control group, whereas they remained constant in the PBM group. At follow-up, a (borderline) significant difference was observed between both groups for the 6MWT and patients’ pain level, in benefit of the PBM group. Their conclusion was this trial shows promising results concerning the prevention of CIPN with PBM in breast cancer patients. Furthermore, a better QoL was observed when treated with PBM. 2
In another study their data indicate that photobiomodulation is an effective, low-toxicity treatment for CIPN. Nearly 90% of patients experience significant improvement in mTNS scores that begins within weeks of initiating treatment and persists for at least 10 weeks after the conclusion of therapy. The benefits appear to accrue similarly to patients with variable duration and intensity of neuropathy symptoms, as well as to patients with variable chemotherapy exposures. Treatment effect lasts well beyond the period of active treatment but diminishes over time, suggesting that further optimization of the treatment algorithm should be explored. 2
Ribbons PT provides cold laser therapy at both Kingsport and Johnson City locations to help providers maintain patients on their prescribed chemotherapy regimen with as little side effects of CIPN as possible. Our results in treating patients suffering CIPN-both during their coarse of chemotherapy and after, have been remarkable. To substantiate perceptions from our patients and staff, we chose to perform an internal review of internal patient records (Timed Up & Go (TUG) assessment, Single Leg Stance Test (SLS), and FACT/GOG-NTX-13) to compare results with published studies and found a striking resemblance.
The Timed Up & Go (TUG) assessment is commonly used to assess patient’s mobility and fall risk. The patient sits back in a chair with arm rests, walk 10 feet, and return to the chair while being timed. Adults who take 12 seconds or longer to complete are at increased risk of falling.
2. The use of photobiomodulation therapy for the prevention of chemotherapy-induced peripheral neuropathy: a randomized, placebo-controlled pilot trial (NEUROLASER trial) Lodewijckx Joy et al

A random sample of our patient’s TUG assessment was averaged with the following results:
- 16 seconds at initial evaluation and 11 seconds at discharge
The Single Leg Stance Test (SLS) is often used to assess static postural control and balance. Balance deficits are common with peripheral neuropathy in the feet due to difficulty determining where the body is positioned in space. A random sample of our patients’ SLS times were averaged at initial evaluation and discharge. See results below:
| Initial Evaluation | right SLS: 6.82 seconds | left SLS: 4.36 seconds |
| Discharge | right SLS: 14.37 seconds | left SLS: 11.49 seconds |
Other treatment options available to medical oncology include gabapentin and cyrocompression.
Gabapentin is prescribed in some cases to address CIPN but with mixed results. Additionally, the side effects as well as stigma of qualifying for schedule V drugs is contraindicated in this patient population.
A gabapentin study of patients with symptomatic CIPN who complained of ‘average’ daily pain scores of either 1) >/=4 on a 0-10 numerical rating scale (NRS); or 2) >/=1 on the 0-3 Eastern Cooperative Oncology Group neuropathy scale (ENS) were eligible (higher numbers indicate greater severity of symptoms in both scales). Patients were randomized to receive gabapentin (target dose, 2700 mg) or placebo for 6 weeks. Crossover occurred after a 2-week washout period. CIPN-related symptoms were evaluated weekly by questionnaires. Statistical methods followed established methods for crossover designs, including Student t tests to compare average intrapatient differences between treatments and linear models to adjust for potential concomitant covariates. Results: There were 115 patients who were randomly assigned to the treatment or control arm. Both groups were well matched by symptoms at study entry. Changes in symptom severity were statistically similar between the 2 groups during the study. Adverse events were mild and similar in both groups. Conclusions: This trial failed to demonstrate any benefit to using gabapentin to treat symptoms caused by CIPN.4
3. The use of photobiomodulation therapy for the prevention of chemotherapy-induced peripheral neuropathy: a randomized, placebo-controlled pilot trial (NEUROLASER trial) Lodewijckx Joy et al
4. Efficacy of gabapentin in the management of chemotherapy-induced peripheral neuropathy: a phase 3 randomized, double-blind, placebo-controlled, crossover trial (N00C3) Ravi D Rao et al

The use of cryotherapy requires individualized care because of differences in cold tolerance. Therefore, a discussion of the risk-benefit ratio is warranted. The use of best practice interventions can successfully manage the discomfort from the freezing temperatures. Finally, safety concerns always remain a priority. The occurrence of a significant association between cold therapy and the frequency and severity of PN and a lack of a relationship between PN and QOL suggests a need for more research. Researchers could more closely scrutinize the interrelationships among cold therapy, CIPN, QOL, and other variables, such as pain and disability, using a path analysis over 12 months following chemotherapy. Between weeks 12 and 16, there was a decline in neuropathy in the SOC group and an increase in neuropathy in the CTG. The possibility that the effects of cold therapy are short-lived and decrease or disappear after 12 weeks requires further longitudinal research over at least one year with a larger sample to discover the answer to this question. 5 In addition to lack of staffing resources necessary to help patients don and doff difficult cold compression garments during infusion is the fact that more and more insurance companies are denying reimbursement for cryocompression due to lack of evidence and improper use of compression billing coding.

In conclusion, if you have patients suffering from CIPN as a result of chemotherapy, whether currently undergoing treatment or post-treatment, you have a source available right now to help them alleviate the pain and fall-risk. By referring them to Ribbons Physical Therapy for cold laser treatment, we can help them with balance and dexterity deficits. Cost for these combined treatments are typical of standard PT/OT visits.
5. Impact of Cold Therapy on Paclitaxel-Induced Peripheral Neuropathy and Quality of Life m Patients With Breast Cancer Mei-Ying Jue et al.
6. AirCast Cryo/Cuff Compression Dressing System
If you desire to receive this newsletter electronically, please let us know:
Email: office@ribbonspt.com